
INTRODUCTION
The number of French workers employed as long-haul transport drivers (LHTDs) exceeds 0.25 million1. Despite the vital contribution of road transport to the stability and growth of the French economy and the EU, the health of LHTDs in France has not received sufficient attention.
LHTDs have increased health risks due to the conditions and vagaries of their work schedule, which frequently result in sleep deprivation and disorders, unhealthy or limited dietary intake, and inadequate exercise2,3. Studies have also found that LHTDs have higher rates of heart disease, diabetes, and lung cancer, associated with obesity, sedentary lifestyles, tobacco consumption, and the use of stimulants4,5. Sieber et al.6 found that obese LHTDs had a smoking prevalence rate that was twice that of the general adult population and over two-thirds of respondents were classified as obese. Other studies have found increased risks among LHTDs for psychiatric and psychological disorders, musculoskeletal disease, and sexually transmitted diseases7-10. High demands and low decision latitude, which typify the work experience of professional drivers, have been associated with an increased risk of myocardial infarction5. Apostolopoulos et al.7 estimated that the life expectancy of male truck drivers was considerably lower than the general population of American men.
Also, studies have shown that obesity may interfere with tasks requiring complex motor skills, concentration and attentive focus such as operating trucks, buses, aircraft, and other transport vehicles. A study conducted in Brazil of 4878 truckers found that increased BMI was significantly associated with shorter sleep duration (<8 hours)11. Also, the U.S. Large Truck Crash Causation Study in a rigorous examination of 963 accidents involving a truck found that 13% were due to exhaustion12.
Research by Anderson et al.13 found that the crash risk for drivers who were defined as obese was significantly higher than those who had normal BMI scores. Further, obesity is a major public health risk that has been strongly linked to increased cardiovascular disease, diabetes mellitus, hypertension and some cancers, as well as other chronic diseases in France and among truck drivers in other countries5,14. A study in 2018 by Carreas-Torres et al.15 found a complex association between obesity and smoking, suggesting that smoking can reduce obesity as an appetite suppressant but at higher levels of obesity can also increase smoking risks and smoking intensity15.
Laws governing intracontinental freight transportation within Europe are regulated by individual countries and the EU. France has one of the highest km/driver ratios due in part to the shortage of drivers, which is expected to increase by 20% over a 10-year period as the profession has less appeal to younger individuals. The shortage of drivers and high turnover rates may indirectly affect the health of workers because of increased pressures to meet delivery timetables and less time for leisure activity16,17.
The aim of this article is to describe the smoking and obesity behaviors of truck drivers in France, both French and other. These findings may be useful in understanding differences and patterns in the use of tobacco products, risks factors for obesity, and the combined health risks for tobacco and obesity, among this group of transport workers.
METHODS
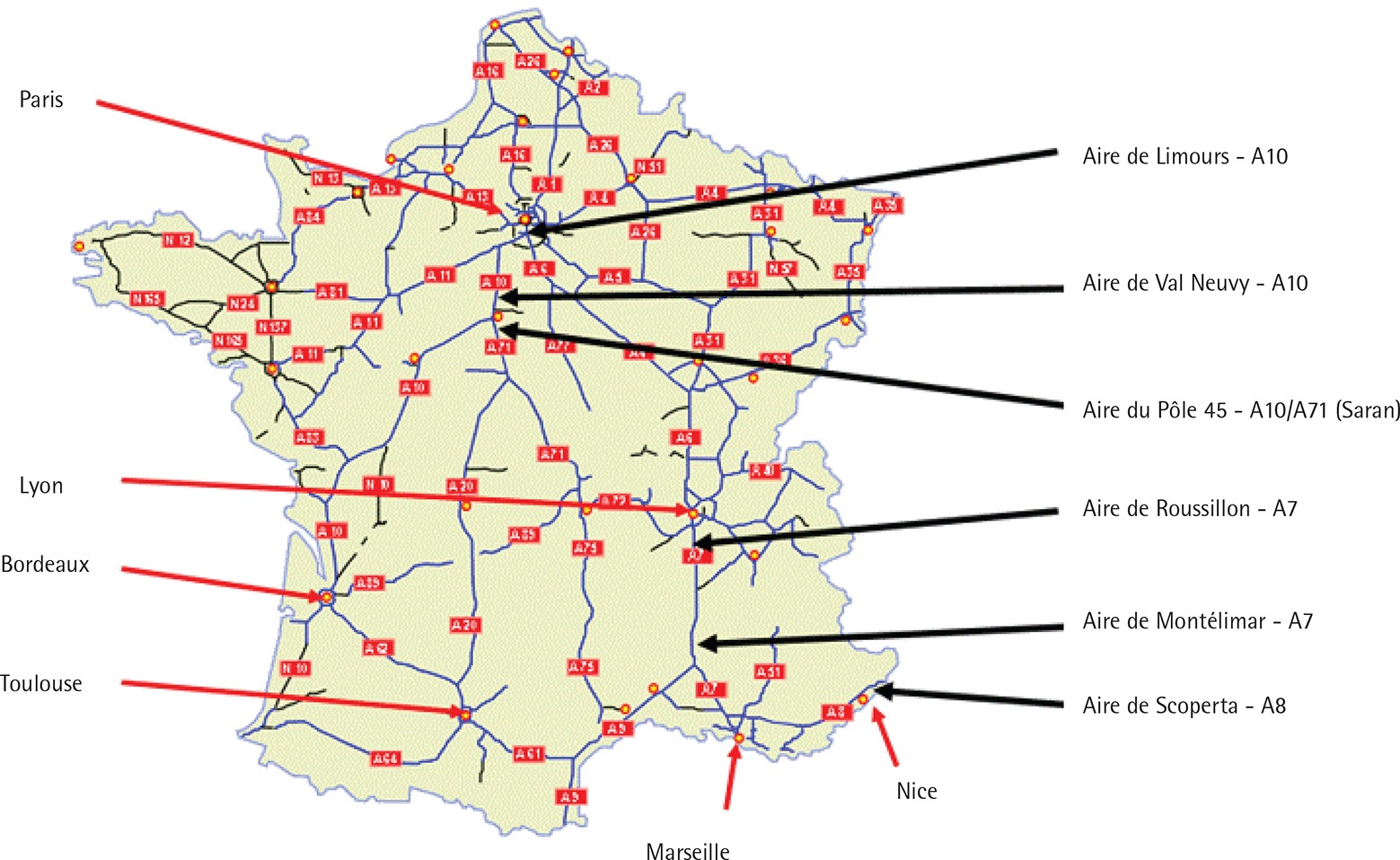
A cross-sectional study was conducted during the Truck Driver Safety Days organized by the nonprofit organization ‘Fondation VINCI Autoroutes pour une Conduite responsable’ on three multiple days during the months of April and October 2012. The duration of the structured anonymous interview was approximately 30 minutes. The survey interviews were conducted using the IPAD 2 (Apple Inc.). The interviews were conducted by trained investigators at six highway rest areas specially designed for professional truck drivers and equipped with shops, restaurants, and lounges [Aire de Roussillon (A7), Aire de Montélimar (A7), Aire de La Scoperta (A8), Aire de Val Neuvy (A10), Aire de Limours (A10), Aire du Pôle 45 – Saran (A10/A71)] (Figure 1). LHTDs were randomly selected and only the driver at the wheel when the truck entered the rest area (between 4 p.m. and 11 p.m.) was interviewed. Each driver selected had the option not to participate in the study. Intercept methods of truck drivers have been employed in a number of other studies to obtain health data from this difficult-to-reach population18-22. A total of 533 drivers were approached and 373 consented, resulting in a sample participation rate of 70%.
Figure 1
French highways, location of the 6 rest areas (Aire de repos) studied and main French cities
Measures
The questionnaire underwent a number of revisions and was pretested with potential respondents. Variables included self-reported sociodemographic characteristics (age, gender, marital status, and nationality), behavioral variables (consumption of sodas, daily exercise, smoking status). The mean age was 43.4 years and the age variable was categorized as: <40, 40–50, >50 years. Nationality referred to French or other EU drivers working in France. Active sports engagement was categorized as active or non-active. The daily use of caffeinated drinks, energy drinks, and sodas was grouped as: 0, 1–2, 3–4, and ≥5 sodas. LHTDs were also asked about the weight of their trucks (≤40 tons or >40 tons), and driving history including any accidents last year (no/yes) and distanced in thousands of km traveled in the last year (<125, 125–150, >150).
Body mass index (BMI) was calculated. BMI (kg/m2) categories were divided into: underweight <18.5, normal ≥18.5 to <25.0, overweight ≥25.0 to <30.0, obese ≥30 to <35, and morbidly obese ≥35. Smoking status was defined as current consumption of tobacco products and respondents were divided into non-smokers and smokers.
Statistical analysis
Continuous variables are presented as frequencies, percentages, and means. The BMI mean and standard deviation were calculated for each behavioral variable and age group. Statistical analysis assessing bivariate associations were conducted using chi-square analysis. Multiple logistic ordinal regression (MLR) models were developed to examine the simultaneous effects of predictor variables on each of the two dependent variables: smoking and BMI, separately and combined. SPSS was used to conduct the analysis.
RESULTS
The mean age of the LHTDs was 43.4 ± 9.7 years, and most (41.2%) were aged 40–50 years, French (70.3%), married (73.8%) and did not report having an active exercise routine (66.0%). Almost an equal proportion of drivers consumed daily 1–2 (34.2%) or 3–4 sodas (33.2%) (Table 1).
Table 1
Sociodemographic and transport variables by Body Mass Index (BMI) and smoking status (%)
| Variables | n (%) | Normal | Overweight | Obese | Morbidly obese | Smokers |
|---|---|---|---|---|---|---|
| Age (years) | ||||||
| <40 | 123 (32.9) | 41.5 | 36.6 | 17.1 | 4.9** | 62.6*** |
| 40–50 | 154 (41.2) | 31.8 | 42.2 | 17.5 | 8.4 | 53.2 |
| >50 | 97 (25.9) | 31.3 | 39.8 | 19.5 | 9.4 | 33.0 |
| Mean ± SD | 43.4 ± 9.7 | |||||
| Nationality | ||||||
| Other | 111 (29.7) | 18.9 | 41.4 | 25.2 | 14.4* | 43.2* |
| French | 263 (70.3) | 36.5 | 39.2 | 17.1 | 7.2 | 54.4 |
| Marital status | ||||||
| Single/unmarried | 98 (26.2) | 35.7 | 38.8 | 16.3 | 9.2 | 60.2* |
| Married | 276 (73.8) | 29.7 | 40.2 | 20.7 | 9.4 | 47.8 |
| Active sport engagement | ||||||
| Yes | 127 (34.0) | 37 | 40.9 | 15 | 7.1 | 48.8 |
| No | 247 (66.0) | 28.3 | 39.3 | 21.9 | 10.5 | 52.2 |
| Number of sodas daily | ||||||
| 0 | 29 (7.8) | 34.5 | 41.4 | 10.3 | 13.8* | 27.6*** |
| 1–2 | 128 (34.2) | 33.6 | 39.1 | 17.2 | 10.2 | 46.1 |
| 3–4 | 124 (33.2) | 26.6 | 40.3 | 24.2 | 8.9 | 50.0 |
| ≥5 | 88 (23.5) | 33 | 40.9 | 19.3 | 6.8 | 68.2 |
| Distance traveled last year (103 km)* | ||||||
| <125 | 183 (50.8) | 32.8 | 40.4 | 22.4 | 4.4* | 50.3 |
| 125–150 | 113 (28.3) | 29.2 | 38.9 | 17.7 | 14.2 | 54.0 |
| >150 | 62 (16.6) | 30.6 | 41.9 | 11.3 | 16.1 | 50.0 |
| Truck weight (tons) | ||||||
| <40 | 37 (9.9) | 40.5 | 43.2 | 10.8 | 5.4 | 64.9 |
| >40 | 337 (90.1) | 30.3 | 39.5 | 20.5 | 9.8 | 49.6 |
| Accidents last year | ||||||
| No | 347 (92.8) | 31.4 | 39.5 | 19.9 | 9.2 | 51.9 |
| Yes | 27 (7.2) | 29.6 | 44.4 | 14.8 | 11.1 | 40.7 |
| BMI (kg/m2) | ||||||
| Normal | 117 (31.3) | 67.5*** | ||||
| Overweight | 149 (39.8) | 44.3 | ||||
| Obese | 73 (19.5) | 43.8 | ||||
| Morbidly obese | 35 (9.4) | 40.0 | ||||
| Mean ± SD | 27.9 ± 4.7 | |||||
| Smoking status | ||||||
| Non-smoker | 183 (48.9) | 20.8 | 45.4 | 22.4 | 11.5*** | |
| Current smoker | 191 (51.1) | 41.4 | 34.6 | 16.8 | 7.3 | |
| Normal BMI/non-smoker | ||||||
| Non-normal BMI and/or smoker | 336 (89.8) | |||||
| Normal BMI and non-smoker | 38 (10.2) | |||||
The majority (50.8%) of the LHTDs drove <125 thousand km annually and more than a quarter (28.3%) drove 125–150 thousand km. A notable proportion (16.6%) of truck drivers exceeded 150 thousand km per year. Most participants drove trucks weighing >40 tons and <10% indicated that they were involved in an accident in the last year.
Based on the BMI categories, respondents were normal (34.3%), overweight (39.8%), obese (19.5%), and morbidly obese (9.4%). The mean BMI was 27.9 ± 4.7 kg/m2. The results revealed that about half of the participants (51.1%) were current or active tobacco users.
Age was significantly related to BMI as older drivers were less likely to have registered a normal BMI (p<0.01). Almost twice as many French respondents compared to their foreign counterparts (36.5% vs 18.9%) registered a normal BMI (p<0.01).
Drivers aged <40 years (62.6%, p<0.001) were more likely to be smokers than either those aged 40–50 years (53.2%) and those aged >50 years (33%), as were French drivers (54.4%, p<0.05) compared to foreign drivers (43.2%). Also, married truckers (60.2%, p<0.05) were more likely to be smokers than non-married (47.8%).
Daily consumption of sodas was significantly (p<0.05) related to BMI, however a clear pattern was not apparent.
More than two-thirds of LHTDs with a normal BMI were significantly more likely to be smokers (67.5%, p<0.001) than those classified as overweight (44.3%), obese (43.8%), or morbidly obese (40.0%). A greater proportion of non-smokers were classified as overweight (45.4%), obese (22.4%), and morbidly obese (11.5%), compared to current smokers (p<0.001).
As shown in Table 2, MLR analysis revealed that the probability of having a normal BMI was significantly associated with age, nationality, and smoking status. Respondents who were aged >50 years were more likely (OR=2.62; 95% CI: 1.24–5.54) to have a normal BMI than those aged <40 years. Also, French LHTDs were considerably more likely (OR=3.04; 95% CI: 1.62–5.69) to report a normal BMI compared to drivers from other European countries. Smokers were significantly more likely than non-smokers (OR=2.12; 95% CI: 0.1.26–3.58) to have an above normal BMI.
Table 2
Logistic regression models for BMI, smoking, BMI and smoking combined
| Normal BMI OR (95% CI) | Smokers OR (95% CI) | Normal BMI/non-smokers OR (95% CI) | |
|---|---|---|---|
| Age (years) | |||
| <40 | 1 | 1 | 1 |
| 40–50 | 1.09 (0.62–1.92) | 0.65 (0.37–1.14) | 1.14 (0.49–2.66) |
| >50 | 2.62 (1.24–5.54)* | 0.24 (0.12–0.46)*** | 0.72 (0.25–2.05) |
| Nationality | |||
| Other | 1 | 1 | 1 |
| French | 3.04 (1.62–5.69)*** | 1.33 (0.78–2.28) | 1.44 (0.62–3.36) |
| Marital status | |||
| Single/unmarried | 1 | 1 | 1 |
| Married | 0.99 (0.56–1.75) | 0.64 (0.37–1.10) | 1.28 (0.55–3.00) |
| Active sports engagement | |||
| No | 1 | 1 | 1 |
| Yes | 1.58 (0.95–2.65) | 1.45 (0.87–2.40) | 0.53(0.26–1.11) |
| Number of sodas daily | |||
| 0 | 1 | 1 | 1 |
| 1–2 | 1.46 (0.56–3.80) | 2.49 (0.95–6.48) | 0.30 (0.10–0.89)* |
| 3–4 | 2.27 (0.85–6.09) | 3.88 (1.46–10.32)** | 0.27 (0.09–0.80)* |
| ≥5 | 1.93(0.70–5.31) | 7.40 (2.66–20.59)*** | 0.11 (0.03–0.44)** |
| Truck weight (tons) | |||
| <40 | 1 | 1 | 1 |
| >40 | 1.81 (0.75–4.36) | 0.34 (0.14–0.83)* | 1.45 (0.31–6.82) |
| Distance traveled last year (103 km) | |||
| <125 | 1 | 1 | 1 |
| 125–150 | 1.01 (0.57–1.78) | 1.34 (0.78–2.31) | 1.71 (0.76–3.86) |
| >150 | 1.03 (0.53–2.02) | 1.08 (0.56–2.08) | 0.98 (0.35–2.71) |
| Accidents last year | |||
| No | 1 | 1 | 1 |
| Yes | 1.39 (0.52–3.71) | 0.45 (0.18–1.14) | 1.23 (0.34–4.48) |
| Smoking | |||
| No | 1 | ||
| Yes | 2.12 (1.26–3.58)** | ||
| BMI | |||
| Normal | 1 | ||
| Overweight | 0.44 (0.25–0.78)** | ||
| Obese | 0.48 (0.24–0.97)* | ||
| Morbidly obese | 0.58 (0.24–1.40) | ||
LHTDs who were aged >50 years were significantly less likely to be smokers compared to those aged <40 years (OR=0.24; 95% CI: 0.12–0.46). LHTDs who daily consumed either 3–4 sodas (OR=3.88; 95% CI: 1.46–10.32) or >5 sodas (OR=7.40; 95% CI: 2.66–20.59) were highly more likely to be smokers than those who reported typically drinking no beverages during the day. Drivers who were overweight or obese were less likely (OR=0.44; 95% CI: 0.25–0.78 and OR=0.48; 95% CI: 0.24–0.97, respectively) to be current smokers than those who had normal BMI values.
In the model predicting a reduced health risk, combining both BMI and smoking status, the number of beverages consumed per day was strongly and significantly associated with a normal BMI and non-smoker status. Respondents who daily consumed either 1–2 (OR=0.30; 95% CI: 0.10–0.89), 2–3 (OR=0.27; 95% CI: 0.09–0.80), or >5 sodas (OR=0.11; 95% CI: 0.03–0.44) were significantly less likely to have a normal BMI and to have abstained from tobacco consumption.
DISCUSSION
As the first study to examine smoking and obesity among LHTDs in France, this work adds considerably to our understanding of the health hazards and potential dangers facing transport workers. These workers are subject to occupational risks including social costs affecting their personal lives and families, and consequentially society at large. These findings may serve as baseline indices to assess progress in improving the health of LHTDs in France, particularly with respect to smoking prevalence and obesity.
In France, the epidemiology of smoking differs from that of the United States where the consumption of tobacco has diminished considerably among all demographic groups and is less than half the prevalence of the French population23. However, the proportion of smokers in the US among LHTDs (51%) reported in a large study by Sieber et al.6 was virtually identical (51.1%) to the rate of smoking found in the present study6. They also found that 68.9% of US LHTDs were obese and 17.4% were morbidly obese. The comparable figures for French truckers in our study were much lower, 17.2% and 7.1%, respectively. Interestingly, young drivers were significantly more likely to be smokers than their older counterparts and this finding was unrelated to nationality. This result has implications for the future health of truckers as the potential occupational longevity of younger drivers may portend cumulative risks for tobacco related illnesses.
Our analysis revealed a statistically significant association between smoking status and beverage consumption. Other studies have shown a positive relationship between caffeine consumption and nicotine consumption, and caffeine use has been shown to increase the likelihood of nicotine dependence using animal models24-27. Coffee and other caffeinated drinks may contain high proportions of sugar and other ingredients that are not conducive to healthy diets and could exacerbate existing health problems24.
Tobacco use has been shown to be correlated with daytime sleepiness in truck drivers and caffeine use has been shown to reduce fatigue and related accidents in truck drivers, which suggests that the use of nicotine and caffeine conjunctively may produce antagonistic effects on sleepiness and sleep-related accidents28,29.
It has been shown that novelty seeking is a predictor of both caffeine and nicotine use and that cocaine users drink more caffeinated beverages per day than the general population, although they are less likely overall to consume caffeinated beverages30,31. Speculatively, it is possible that caffeinated beverage consumption acts as a predictor of addictive behaviors and that those who consume a variety of caffeinated beverages are also more likely to engage in the use of stimulants, irrespective of outside factors. Although beyond the scope of this study, future studies may benefit from the exploration of caffeinated beverage consumption in relation to illicit drug use among transport workers.
BMI was found to be related to the nationality and smoking status, which may have moderated obesity in this sample of LHTDs, as smoking cigarettes is an appetite suppressant32. It is not surprising that the BMI of French truck drivers was much lower than those of other nationality LHTDs. Also, somewhat speculatively, the cultural influence of dietary habits and nutrition on other nationality LHTDs could account for differences in obesity prior to their employment as French truckers. Moreover, the combined health effects of cigarette consumption and obesity increase the likelihood of negative health consequences.
Public policy monitoring and controlling the work schedules, conditions, and health requirements of LHTDs in France are determined both by national and EU deliberations and dictates. Although the EU has several umbrella regulations governing its member states with respect to driving hours (e.g. daily driving period shall not exceed 9 hours) and rest periods (e.g. daily rest period shall be at least 11 hours), there are no standard health guidelines, minimal criteria, or systemic means of monitoring the health of its drivers33. Restrictions on LHTDs in France are more stringent than in the EU (e.g. highly restrictive driving on Sunday or holidays, restricted speed limits, mandatory stops every 4.5 hours for at least 45 minutes). Also, in France, medical exams are required to obtain a long-haul truck driving license, and periodic exams are required every 5 years, at 60 years every two years, and at 60–76 years every year, and every year thereafter for those aged >76 years34.
More importantly, at present, there is a paucity of preventive health programs addressing the needs and problems of LHTDs in France. A comprehensive wellness programs, voluntary or otherwise, consisting of health education modules, exercise, and literature aimed at reducing obesity and tobacco consumption, and other health topics at rest stops or in companies, could potentially save lives and benefit employees, employers, and the society at large35,36. For example, in their systematic review of prevention programs for truck drivers, Ng et al.35 found that interventions resulting in statistically significant BMI improvements not only focused on individuals but also included modules such as group education/counseling and theory-based strategies (e.g. stages of change theory). Their analysis also revealed that two smoking cessation programs yielded significant reductions in tobacco use among LHTDs36.
Limitations
This study is limited by the small sample size of 374 participants, of whom about 30% were non-native French transport workers. Future studies of this population should include a larger number of participants and more varied methods of data collection. Additionally, self-reported information about personal health behavior is always subject to some form of bias. The use of objective indices (e.g. biochemical validation, weight/height scales) could reduce bias. Also intercept studies, while quite useful in reaching difficult to study groups such as LHTDs, are intrinsically problematic as noted by Sieber et al.6 because they miss drivers who are unavailable due to vacations, work schedules, illness or other reasons for not working. Some study variables including tobacco consumption, use of caffeinated drinks and alcohol, sleeping habits, exercise, and other behaviors and risks were not measured in sufficient detail to adequately determine frequency and other attributes.
CONCLUSIONS
LHTDs provide an essential societal function in transporting a nation’s goods and products daily under occupational conditions that can be vastly improved, particularly with respect to health and medical consequences. Maintaining a healthy and alert workforce of LHTDs can also improve the highway safety of the general population by reducing vehicle accidents involving LHTDs, which have higher fatality rates. This study points to the need to address health risks associated with smoking and obesity of LHTDs in France. In this regard, a multifaceted set of strategies should be considered entailing empirical studies focusing on specific health risks and medical problems; designing, implementing, and evaluating interventions in collaboration with drivers, unions, and employers; improving the challenging working and structural conditions of long-haul trucking under which drivers worked; and legislative initiatives that protect and enhance the health of LHTDs.